Vision falls after laser vision correction - what to do? Or, doctor, make me an "enhancement"
Traditionally, this is the most frequent question for those who have already made a correction and for those who are just planning it. Let us agree that the word “falls” will mean a change in the optics of the eye — that is, an increase in minus, astigmatism, or the appearance of a plus. In short, when you need glasses again to see well. Or lenses. Or, again, a correction, more precisely, an additional correction. By the way, in English medicine this term sounds much more pleasant - “enhancement” - improvement, improvement.
Since the deterioration / fall in vision may be due to other causes - diseases of the retina, optic nerve, lens, eye surface, etc., they must first be excluded. Then optics has nothing to do with it and the main disease should be treated.
So, enhancement is an additional correction. Is it always possible?
Much depends on what method you first made the correction, for example, it was ReLEX SMILE, LASIK or keratotomy (notches). The choice of improving technology will differ depending on the surgeon - his hands and professional intelligence, on the type and model of the laser, on your individual characteristics of the organism, etc. In short, for a patient as a game of "poker" - with fully or partially closed cards, in which elements of all species are combinations. About correction methods written HERE .
There are many methods - I give navigation by choice of the necessary. Arm yourself.

For medical reasons, we can speak about the correction of vision when we have an increase in the axial length of the eye, regression after correction, or residual unplanned refraction (optics).
Most often we are talking about this not earlier than 3 months after the correction - this increases its accuracy.
Important:
In short, this is similar to “poker” - a lot of combinations, the patient and the surgeon do not have complete information (often additional correction is done after years, in another clinic), “trading” is possible in the selection process. This is not a chess game in which both players see the position of all the pieces on the board.

The method is the most modern, the most accurate and most gentle with proper performance. On him the most questions and myths. What is its fundamental difference written in these articles: "Direct comparison of laser correction methods for myopia" and "Why we make SMILE"
For SMILE, you can use the largest range of possible corrective measures:
1. SMILE after SMILE (Sub-cap lenticule extraction)
If we are talking about myopia and astigmatism, then we can perform the additional correction using the same SMILE method. Schematically it looks like this:
This method can also be used to correct myopia for more than 10 diopters (for example, -15.0 diopters) - in the form of a two-step procedure. Method for highly experienced ReLEX SMILE surgeons who have experience with thin lentikuly.
Is it possible to do this in the same 2 mm? Easy - I'm the second stage I use the same input size of 2 mm! But this should also be sufficient thickness of the cornea, as well as for the correction in general.
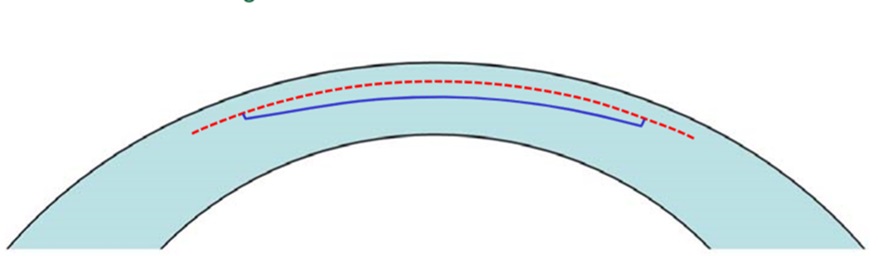
2. Formation of the edge cut (side cut) for the formation of the valve cover (flap) is a kind of transition to femtoLASIK technology with a lid equal to the diameter of the “cap” at SMILE. It looks like this:
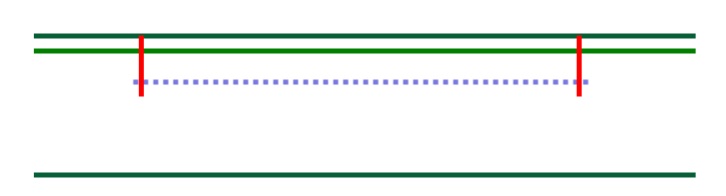
It can be used if it is calculated that at least 300 microns remain under the lid. The diameter of the cover should be sufficient, and how much the thickness of the cover in this case does not matter.

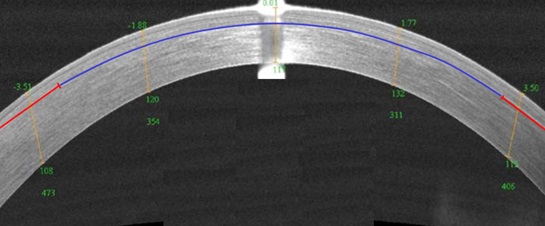
Cornea tomogram after formation of the marginal cut
3. CIRCLE is a program that also allows you to create a valve cover (flap) and switch to femtoLASIK technology with a lid of a larger diameter than the diameter of the cap. This is a regular, recommended by the manufacturer module for the correction. The module is very useful, though Zeiss does not give everyone access to it at once.
Schematically it looks like this:
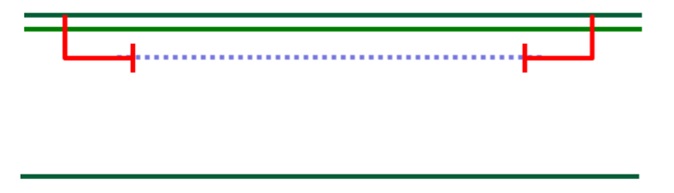
The cover rises and excimer laser polishing is done. What is its advantage? This is necessary to obtain a large-diameter optical zone = high-quality vision.
Therefore, I often in the case of additional correction of “alien” eyes after femtoLASIK (if the diameter allows) use CIRCL to create a new side cut with a smooth edge.
So on the tomogram looks like the cornea after CIRCLE
Schematic difference SMILE and CIRCLE
Performing this procedure also requires applying a vacuum cone and a laser operating time of about 15 seconds.
Why is the safety of the transition from SMILE to femtoLASIK, if necessary for additional correction, higher than the rise of the already formed lid after femtoLASIK and the repeated additional correction?
Hence, the quality of vision after such a correction after SMILE is higher than the same correction after a femtoLASIK.

This is how the surface of the eye looks like under a microscope 10 minutes after CIRCLE
4. FemtoLASIK (Thin Flap LASIK) above SMILE.
If you perform a ReLEX SMILE at a depth of at least 135 microns, then you can use a “cap” (cap) to form a thin top cover.
And then everything is as usual - we open the lid, evaporate as much as necessary and how much the thickness of the cornea from the bottom allows, close the lid. Schematically looks like this:
Tomogram of the cornea after the formation of a thin cap in the "cap" SMILE

The eye looks great and the vision is 1.0
5. FemtoLASIK (Thick Flap LASIK) at the bottom SMILE.
If you perform a ReLEX SMILE at a depth of 100 microns, then in this case you can use the lower part of the cornea to form a thick top cover that includes the SMILE area. And then everything is as usual - we open the lid, evaporate as much as necessary and how much the thickness of the cornea from the bottom allows, close the lid. Schematically looks like this:
6. The PRK method (or transFRC) - we can use it with a final cornea thickness of more than 350 microns.
Of course, he has all the disadvantages of PRK:
On the left - transFRK, on the right - classic PRK
7. Intrastromal keratoplasty (intrastromal keratotomy) - using a femtosecond laser, you can make incisions in the stroma, thereby changing the curvature of the cornea. Such a modern modification of ancient keratotomy.
Of the benefits - there is no loss of corneal tissue, there is no damage to the front surface of the cornea.
Schematically looks like this:
8. Implantation of a phakic IOL.
How this is done can be read here: "Calculation of intraocular phakic lenses . "
If there is enough space in the posterior chamber of the eye - more than 3 mm, then a phakic correction lens can be implanted, which does not need to be removed and apparently it is not visible at all. Then we do not touch the cornea, and leave our lens. Only something useful is placed in the eye.
The previously performed correction in the cornea does not in any way interfere with the calculations of the phakic IOL or its implantation.

Diagram of implantation of phakic intraocular lens
1. Raising the lid.
The important point is that in the cornea there is already a surface flap of a certain thickness that is a flap. This operation differs from the LASIK correction method only in that the surgeon picks up a flap of the cornea, which was cut off earlier, and does not cut it off again. It is held only by the epithelium in the case of LASIK, and the “epithelium + edge of the lid” after femtoLASIK.
The lid itself never grows - even after a few decades it can be lifted, but never the edges after lifting remain as smooth as the primary ones.
And making the primary correction is always easier than any additional correction.

The procedure for the formation of the valve cover with LASIK
After LASIK, it is often possible to lift the old lid with a single spatula movement, after femtoLASIK it takes more effort. This is both good and bad - something that rises easily, moves easily (for example, in case of injury) and vice versa.
Eye after lifting the lid
Before additional correction, it is necessary to determine the thickness of the previously formed lid and the thickness of the intended cornea remnant in order not to get keratoectasia, I wrote about it here: “Keratoectasia (keratoconus,“ convex cornea ”): what is it and what to do about it . ”
After femtoLASIK, the edge of the lid is held tight, therefore, in order not to injure it, you can resort to forming a new marginal entrance (side cut) with the help of CIRCLE.
Risks to raise the interface:
In short, there is no cover - there are no problems with the cover: for this you need to choose premium SMILE or low-cost transFRK.
2. SMILE in the "lid"
This technology can be done only if the cap is thick - old corrections with the first models of keratomes cut the caps up to 200 microns thick. Of the benefits - since the lid is cut off, it does not add strength, changing its thickness does not affect the overall strength of the cornea, and SMILE only 25 seconds, the next day there are no restrictions, we don’t lift anything, the epithelium does not grow, the biomechanics doesn’t suffer etc. I used this technique a couple of times.
Here is a diagram of the operation:
3. SMILE under the "cover"
If the cap is thin, the cornea is thick under it - you can make it. In this case, the biomechanics as usual decreases, but again only 25 seconds, the next day there are no restrictions, we don’t lift anything, the epithelium does not grow.
Schematically looks like this:
:) And yes, attentive noticed that the pictures were repeated as in the section on SMILE!
4. PRK / TransFRK
We work according to the usual program - we remove the epithelium, evaporate, process, put on a contact lens, wait for healing and remodeling of the epithelium.
There are also limitations for this method - when we calculate the dioptries that need to be adjusted, we must calculate the thickness of the tissues for evaporation. Fully cover the lid can not be burned - so here the possibilities are limited by the thickness of the lid already!
5. Phakichnaya IOL - one should not forget about it, especially in those cases when you don’t want to touch and thin the cornea, but you need to make a correction.
The method is old, I wrote about it including here.
Therefore, patients after such correction abound. A lot of those who have a characteristic Haze - "nebula" in the cornea, reducing visual acuity and uncorrectable glasses.

This is what the installation for excimer laser correction LASIK and transFRK looks like.
You can offer several options - but all this taking into account the residual thickness of the cornea:
1. ReLEX SMILE
I suggest it if the cornea is thick enough and the cornea is sufficiently transparent (a light haze is not a hindrance). Recovery is extremely fast - as after the standard ReLEX SMILE, even tears are smaller.
2. Repeated PRK - all according to the traditional scenario: removal of the epithelium, work with an excimer laser on the surface of the stroma, surface treatment with a preparation, contact lens for several days. It is better to use it as a method for dealing with the same haze, and with small corrections of up to 1-2 diopters.
3. FemtoLASIK or LASIK - you can cut the lid, lift and evaporate the desired profile. LASIK in this case is an order of magnitude more dangerous - on the flat cornea the lid may be defective.
4. Phakic IOL - again, if there is a place in the back chamber of the eye, and the cornea is small.
From past articles ( “The history of vision correction operations” , “The story about one eye and 20 operations (not readable)” ), we remember that this is the oldest method of the 80s of the last century. Accordingly, most people who have undergone radial keratotomy far in 40-45 years. At the same time, the cornea looks like this - like a pie cut (not through) into pieces, the direction of which coincides with the imaginary radii of the conditional cornea circumference at the central zone with a diameter of at least 3 mm.
Most often we are faced with the appearance of farsightedness - the so-called hypermetropic shift (+) or astigmatism (±). Less often, I have to do an additional correction of myopia (-).
If the lens is transparent and in good condition, choose:
1. FemtoLASIK or LASIK
The operation of choice, since the thickness of the lid is precisely specified and does not allow the cornea to disperse "at the seams". And if in some place it creeps away, then I collect such “petals”. There are surgeons who think that it is risky - the flap will not rise on spikes or fall apart. And choose a much more risky and less desirable LASIK.
LASIK - the formation of a lid by a microkeratome - a mechanism with blades - here it may not sit down as it should, it can turn out to be a “microflap” or “pizza”, but the blade cuts scars easily.
In addition, with femtasic, the rise in intraocular pressure is moderate, much lower than with LASIK vacuum technology.
Thus, we can correct myopia, hyperopia and astigmatism after radial keratotomy.
2. Tightening seams
Over time, the cornea under the action of intraocular pressure and its reduced stiffness sags, the lower scars stretch and fill the epithelium. Like striae on the skin. It looks like this and leads to hypermetropia and astigmatism:
In this case, you can “clean” the epithelium from keratotomy scars, pull them off with thin threads and thus get a “steeper” and more correct cornea. It looks like this:

3. Phakic IOL - We put something useful in the eye as described above.
4. Photorefractive keratectomy - PRK or transFRK.
Perform preferably on topographic profile and just need a cytostatic to the surface. Without mitomycin in such eyes, the development of hayz (subepithelial opacities) is practically through one (and this does not depend on the type of laser). And, of course, all the shortcomings of the PRK will be present - without them in any way.
5. Replacing your own lens with an intraocular lens with new optical parameters , for example, with astigmatism correction, if opacities appear in the lens - a cataract or marked sclerosis begins. Therefore, the state of one’s own lens will play a big role in the choice of methodology - they will not be sorry for it and will propose to solve the problem of correction by replacing the lens with an artificial transparent lens with new optical properties.
Each clinic has its own rules. Our cost of laser vision correction includes a year of postoperative observation and free pre-correction for medical reasons if necessary (though I didn’t have to do it for the last 2,000 eyes even once). If the correction was made in another clinic, and the patient came to me, then it is paid depending on the chosen correction method.
Correction or enchancement is a procedure for changing the optical power of the eye after a previously performed vision correction.
Correction is a good way to improve vision. Each method of correction and pre-correction is chosen on the basis of taking into account a large number of factors, the surgeon's factor is undoubtedly important, the individual parameters of the patient are definitely important, the choice of the clinic is the determining factor. Each method is good, but in order to make the right choice, the surgeon must master the whole range of operations. Otherwise, you will be offered a discount only the available method (in most cases it will be LASIK).
The ReLEX SMILE method is not only fast, but it also gives the least need for additional correction and the largest field for creativity - much more than its predecessors. It can also be used for correction after using other methods!
Since the deterioration / fall in vision may be due to other causes - diseases of the retina, optic nerve, lens, eye surface, etc., they must first be excluded. Then optics has nothing to do with it and the main disease should be treated.
So, enhancement is an additional correction. Is it always possible?
Much depends on what method you first made the correction, for example, it was ReLEX SMILE, LASIK or keratotomy (notches). The choice of improving technology will differ depending on the surgeon - his hands and professional intelligence, on the type and model of the laser, on your individual characteristics of the organism, etc. In short, for a patient as a game of "poker" - with fully or partially closed cards, in which elements of all species are combinations. About correction methods written HERE .
There are many methods - I give navigation by choice of the necessary. Arm yourself.
ENHANCEMENT - additional correction after laser correction already performed - the essence of the matter
For medical reasons, we can speak about the correction of vision when we have an increase in the axial length of the eye, regression after correction, or residual unplanned refraction (optics).
Most often we are talking about this not earlier than 3 months after the correction - this increases its accuracy.
Important:
- Each correction method has its own capabilities - this affects the choice.
- Each surgeon has certain skills - this affects the choice.
- Each clinic has a certain type of equipment - this affects the choice.
- Each patient has individual anatomical initial data and visual needs - this affects the choice, etc.
In short, this is similar to “poker” - a lot of combinations, the patient and the surgeon do not have complete information (often additional correction is done after years, in another clinic), “trading” is possible in the selection process. This is not a chess game in which both players see the position of all the pieces on the board.
Finishing methods after RELEX SMILE or CMILE
The method is the most modern, the most accurate and most gentle with proper performance. On him the most questions and myths. What is its fundamental difference written in these articles: "Direct comparison of laser correction methods for myopia" and "Why we make SMILE"
For SMILE, you can use the largest range of possible corrective measures:
1. SMILE after SMILE (Sub-cap lenticule extraction)
If we are talking about myopia and astigmatism, then we can perform the additional correction using the same SMILE method. Schematically it looks like this:
This method can also be used to correct myopia for more than 10 diopters (for example, -15.0 diopters) - in the form of a two-step procedure. Method for highly experienced ReLEX SMILE surgeons who have experience with thin lentikuly.
Is it possible to do this in the same 2 mm? Easy - I'm the second stage I use the same input size of 2 mm! But this should also be sufficient thickness of the cornea, as well as for the correction in general.
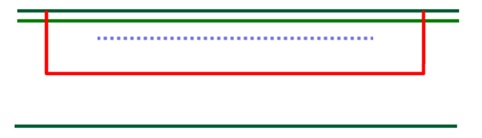
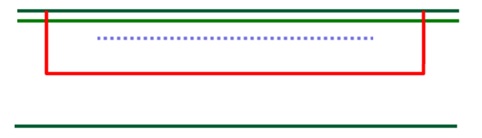
2. Formation of the edge cut (side cut) for the formation of the valve cover (flap) is a kind of transition to femtoLASIK technology with a lid equal to the diameter of the “cap” at SMILE. It looks like this:
It can be used if it is calculated that at least 300 microns remain under the lid. The diameter of the cover should be sufficient, and how much the thickness of the cover in this case does not matter.
Cornea tomogram after formation of the marginal cut
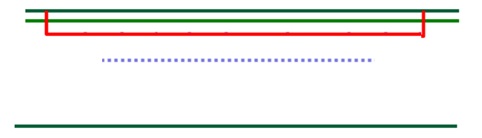
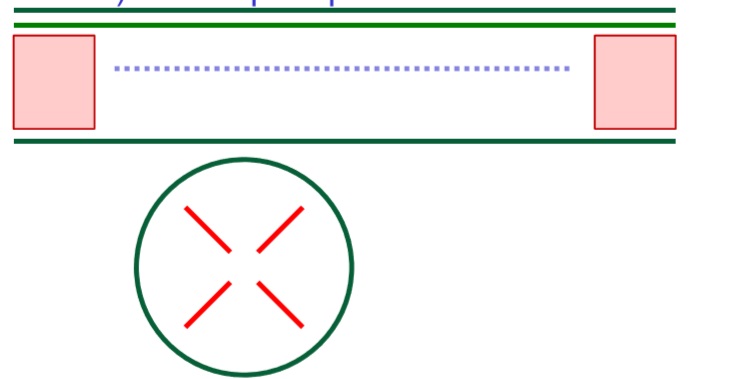
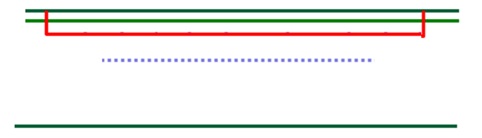
3. CIRCLE is a program that also allows you to create a valve cover (flap) and switch to femtoLASIK technology with a lid of a larger diameter than the diameter of the cap. This is a regular, recommended by the manufacturer module for the correction. The module is very useful, though Zeiss does not give everyone access to it at once.
Schematically it looks like this:
The cover rises and excimer laser polishing is done. What is its advantage? This is necessary to obtain a large-diameter optical zone = high-quality vision.
Therefore, I often in the case of additional correction of “alien” eyes after femtoLASIK (if the diameter allows) use CIRCL to create a new side cut with a smooth edge.
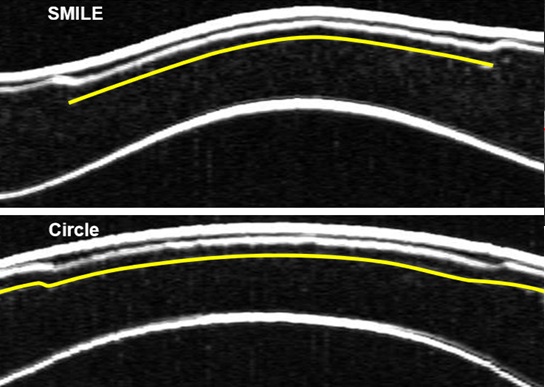
So on the tomogram looks like the cornea after CIRCLE
Schematic difference SMILE and CIRCLE
Performing this procedure also requires applying a vacuum cone and a laser operating time of about 15 seconds.
Why is the safety of the transition from SMILE to femtoLASIK, if necessary for additional correction, higher than the rise of the already formed lid after femtoLASIK and the repeated additional correction?
- because CIRCL allows you to expand the zone for correction, and you will not increase the already made cover;
- when we re-lift the lid (after femtoLASIK or LASIK), the edges become less even and the risk of epithelium growing from the surface under the lid increases, and CIRCLE allows you to create a clear adaptive primary edge.
Hence, the quality of vision after such a correction after SMILE is higher than the same correction after a femtoLASIK.
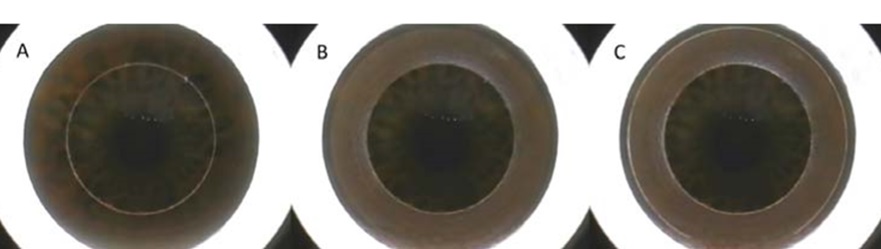
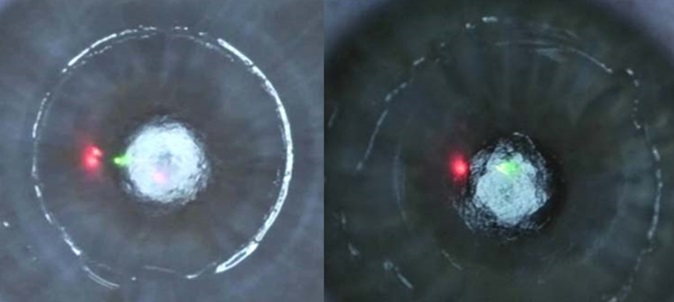
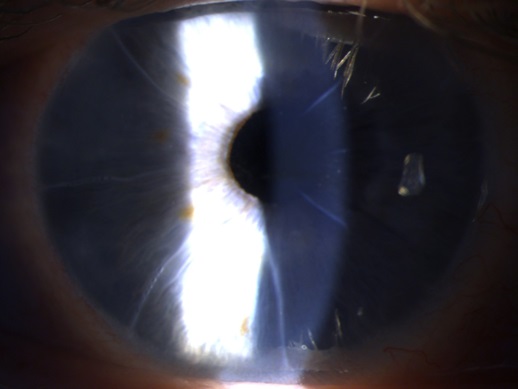
This is how the surface of the eye looks like under a microscope 10 minutes after CIRCLE
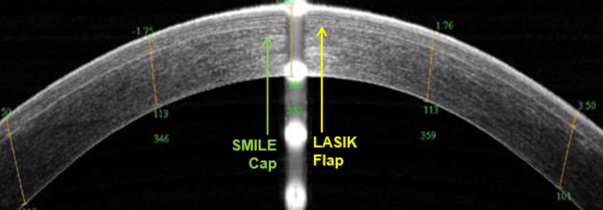
4. FemtoLASIK (Thin Flap LASIK) above SMILE.
If you perform a ReLEX SMILE at a depth of at least 135 microns, then you can use a “cap” (cap) to form a thin top cover.
And then everything is as usual - we open the lid, evaporate as much as necessary and how much the thickness of the cornea from the bottom allows, close the lid. Schematically looks like this:
Tomogram of the cornea after the formation of a thin cap in the "cap" SMILE
The eye looks great and the vision is 1.0
5. FemtoLASIK (Thick Flap LASIK) at the bottom SMILE.
If you perform a ReLEX SMILE at a depth of 100 microns, then in this case you can use the lower part of the cornea to form a thick top cover that includes the SMILE area. And then everything is as usual - we open the lid, evaporate as much as necessary and how much the thickness of the cornea from the bottom allows, close the lid. Schematically looks like this:
6. The PRK method (or transFRC) - we can use it with a final cornea thickness of more than 350 microns.
Of course, he has all the disadvantages of PRK:
- soreness for several days
- risk of heyz
- slow recovery of vision up to several weeks
- the starting (initial) hypermetropic overcorrection associated with epithelial remodeling.
On the left - transFRK, on the right - classic PRK
7. Intrastromal keratoplasty (intrastromal keratotomy) - using a femtosecond laser, you can make incisions in the stroma, thereby changing the curvature of the cornea. Such a modern modification of ancient keratotomy.
Of the benefits - there is no loss of corneal tissue, there is no damage to the front surface of the cornea.
Schematically looks like this:
8. Implantation of a phakic IOL.
How this is done can be read here: "Calculation of intraocular phakic lenses . "
If there is enough space in the posterior chamber of the eye - more than 3 mm, then a phakic correction lens can be implanted, which does not need to be removed and apparently it is not visible at all. Then we do not touch the cornea, and leave our lens. Only something useful is placed in the eye.
The previously performed correction in the cornea does not in any way interfere with the calculations of the phakic IOL or its implantation.
Diagram of implantation of phakic intraocular lens
Advanced correction methods after LASIK / femtoLASIK - technologies with a “lid”
1. Raising the lid.
The important point is that in the cornea there is already a surface flap of a certain thickness that is a flap. This operation differs from the LASIK correction method only in that the surgeon picks up a flap of the cornea, which was cut off earlier, and does not cut it off again. It is held only by the epithelium in the case of LASIK, and the “epithelium + edge of the lid” after femtoLASIK.
The lid itself never grows - even after a few decades it can be lifted, but never the edges after lifting remain as smooth as the primary ones.
And making the primary correction is always easier than any additional correction.
The procedure for the formation of the valve cover with LASIK
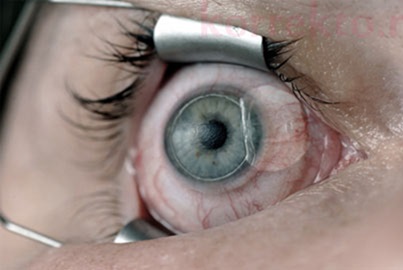
After LASIK, it is often possible to lift the old lid with a single spatula movement, after femtoLASIK it takes more effort. This is both good and bad - something that rises easily, moves easily (for example, in case of injury) and vice versa.
Eye after lifting the lid
Before additional correction, it is necessary to determine the thickness of the previously formed lid and the thickness of the intended cornea remnant in order not to get keratoectasia, I wrote about it here: “Keratoectasia (keratoconus,“ convex cornea ”): what is it and what to do about it . ”
After femtoLASIK, the edge of the lid is held tight, therefore, in order not to injure it, you can resort to forming a new marginal entrance (side cut) with the help of CIRCLE.
Risks to raise the interface:
- with growing under the cover of the epithelium (outer rapidly breeding layer) - because the old edges will not fit as closely as during the initial cut,
- can damage the lid,
- creases of the lid may interfere with vision.
- sometimes you have to deal with a primary wrinkled lid after the first correction, which has not been sufficiently smoothed. Then it is a whole story with the removal of the epithelium, soaking, sewing on the edges as in keratoplasty.
In short, there is no cover - there are no problems with the cover: for this you need to choose premium SMILE or low-cost transFRK.
2. SMILE in the "lid"
This technology can be done only if the cap is thick - old corrections with the first models of keratomes cut the caps up to 200 microns thick. Of the benefits - since the lid is cut off, it does not add strength, changing its thickness does not affect the overall strength of the cornea, and SMILE only 25 seconds, the next day there are no restrictions, we don’t lift anything, the epithelium does not grow, the biomechanics doesn’t suffer etc. I used this technique a couple of times.
Here is a diagram of the operation:
3. SMILE under the "cover"
If the cap is thin, the cornea is thick under it - you can make it. In this case, the biomechanics as usual decreases, but again only 25 seconds, the next day there are no restrictions, we don’t lift anything, the epithelium does not grow.
Schematically looks like this:
:) And yes, attentive noticed that the pictures were repeated as in the section on SMILE!
4. PRK / TransFRK
We work according to the usual program - we remove the epithelium, evaporate, process, put on a contact lens, wait for healing and remodeling of the epithelium.
There are also limitations for this method - when we calculate the dioptries that need to be adjusted, we must calculate the thickness of the tissues for evaporation. Fully cover the lid can not be burned - so here the possibilities are limited by the thickness of the lid already!
5. Phakichnaya IOL - one should not forget about it, especially in those cases when you don’t want to touch and thin the cornea, but you need to make a correction.
Methods of correction after photorefractive keratectomy - PRK / TRANSFRK
The method is old, I wrote about it including here.
Therefore, patients after such correction abound. A lot of those who have a characteristic Haze - "nebula" in the cornea, reducing visual acuity and uncorrectable glasses.
This is what the installation for excimer laser correction LASIK and transFRK looks like.
You can offer several options - but all this taking into account the residual thickness of the cornea:
1. ReLEX SMILE
I suggest it if the cornea is thick enough and the cornea is sufficiently transparent (a light haze is not a hindrance). Recovery is extremely fast - as after the standard ReLEX SMILE, even tears are smaller.
2. Repeated PRK - all according to the traditional scenario: removal of the epithelium, work with an excimer laser on the surface of the stroma, surface treatment with a preparation, contact lens for several days. It is better to use it as a method for dealing with the same haze, and with small corrections of up to 1-2 diopters.
3. FemtoLASIK or LASIK - you can cut the lid, lift and evaporate the desired profile. LASIK in this case is an order of magnitude more dangerous - on the flat cornea the lid may be defective.
4. Phakic IOL - again, if there is a place in the back chamber of the eye, and the cornea is small.
Radial keratotomy - notch technique (manual, nonlaser method)
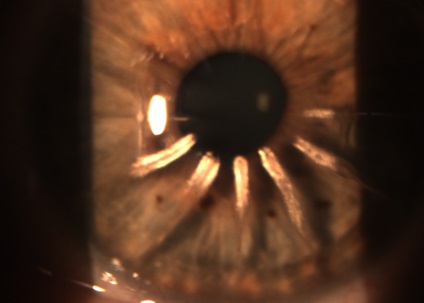
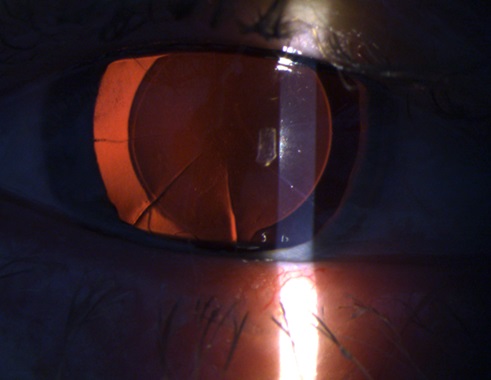
From past articles ( “The history of vision correction operations” , “The story about one eye and 20 operations (not readable)” ), we remember that this is the oldest method of the 80s of the last century. Accordingly, most people who have undergone radial keratotomy far in 40-45 years. At the same time, the cornea looks like this - like a pie cut (not through) into pieces, the direction of which coincides with the imaginary radii of the conditional cornea circumference at the central zone with a diameter of at least 3 mm.
Most often we are faced with the appearance of farsightedness - the so-called hypermetropic shift (+) or astigmatism (±). Less often, I have to do an additional correction of myopia (-).
If the lens is transparent and in good condition, choose:
1. FemtoLASIK or LASIK
The operation of choice, since the thickness of the lid is precisely specified and does not allow the cornea to disperse "at the seams". And if in some place it creeps away, then I collect such “petals”. There are surgeons who think that it is risky - the flap will not rise on spikes or fall apart. And choose a much more risky and less desirable LASIK.
LASIK - the formation of a lid by a microkeratome - a mechanism with blades - here it may not sit down as it should, it can turn out to be a “microflap” or “pizza”, but the blade cuts scars easily.
In addition, with femtasic, the rise in intraocular pressure is moderate, much lower than with LASIK vacuum technology.
Thus, we can correct myopia, hyperopia and astigmatism after radial keratotomy.
2. Tightening seams
Over time, the cornea under the action of intraocular pressure and its reduced stiffness sags, the lower scars stretch and fill the epithelium. Like striae on the skin. It looks like this and leads to hypermetropia and astigmatism:
In this case, you can “clean” the epithelium from keratotomy scars, pull them off with thin threads and thus get a “steeper” and more correct cornea. It looks like this:
3. Phakic IOL - We put something useful in the eye as described above.
4. Photorefractive keratectomy - PRK or transFRK.
Perform preferably on topographic profile and just need a cytostatic to the surface. Without mitomycin in such eyes, the development of hayz (subepithelial opacities) is practically through one (and this does not depend on the type of laser). And, of course, all the shortcomings of the PRK will be present - without them in any way.
5. Replacing your own lens with an intraocular lens with new optical parameters , for example, with astigmatism correction, if opacities appear in the lens - a cataract or marked sclerosis begins. Therefore, the state of one’s own lens will play a big role in the choice of methodology - they will not be sorry for it and will propose to solve the problem of correction by replacing the lens with an artificial transparent lens with new optical properties.
Now about the cost of correction
Each clinic has its own rules. Our cost of laser vision correction includes a year of postoperative observation and free pre-correction for medical reasons if necessary (though I didn’t have to do it for the last 2,000 eyes even once). If the correction was made in another clinic, and the patient came to me, then it is paid depending on the chosen correction method.
Conclusion
Correction or enchancement is a procedure for changing the optical power of the eye after a previously performed vision correction.
Correction is a good way to improve vision. Each method of correction and pre-correction is chosen on the basis of taking into account a large number of factors, the surgeon's factor is undoubtedly important, the individual parameters of the patient are definitely important, the choice of the clinic is the determining factor. Each method is good, but in order to make the right choice, the surgeon must master the whole range of operations. Otherwise, you will be offered a discount only the available method (in most cases it will be LASIK).
The ReLEX SMILE method is not only fast, but it also gives the least need for additional correction and the largest field for creativity - much more than its predecessors. It can also be used for correction after using other methods!
Source: https://habr.com/ru/post/439348/